 Call for an Appointment
Call for an Appointment 






What is it?
Failure of the Achilles tendon to repair itself following injury. The Achilles tendon is the largest tendon in the body which connects the calf muscle to the heel. It may be Insertional (where it inserts into the heel bone) or Non-Insertional (in the mid portion of the tendon).
What causes it?
Repetitive stress to the tendon causing an ‘overuse injury’. This may be due to a sudden increase in activity or tight calf muscles placing extra strain on the tendon. Microscopic tears are produced and the body attempts to heal these with a painful inflammatory response.
What are the symptoms?
Pain in the tendon (Non-Insertional) or the heel (Insertional), in the morning or on activity. Pain the day after exercise. Due to chronic inflammation, the tendon may become thickened due to scar tissue or calcium deposits. If you experience a sudden painful ‘pop’ in the back of your calf or heel, you may have ruptured (torn) your Achilles tendon. You should see Mr Gordon immediately.
How is it diagnosed?
Mr Gordon will take a thorough history and examination and perform radiographs (x-rays) and this is normally sufficient to make a diagnosis. It is important to rule out other problems, which is why a review by an experienced foot and ankle specialist is often necessary. Sometimes the diagnosis may not be clear and an ultrasound or MRI scan may be required.
How is it treated?
There are a host of treatments purported to be of benefit in Achilles tendinopathy, many have very little scientific evidence to support their use. Mr Gordon will recommend evidence based treatments for you and if these do not work, he will discuss with you other options, which may not have such strong scientific evidence, but are worth trying, after informed consent.
Activity Modification
In the first instance, treatment is by modifying your activities that are painful and taking anti inflammatory tablets (Ibuprofen, Diclofenac). Ice packs can also give relief.
Eccentric Stretching Protocol
These are the most important exercise to do, performed under the guidance of a musculoskeletal physiotherapist. The aim is to stretch the Achilles tendon. Expect some discomfort and continue through it, unless severe. The protocol will gradually get harder as you get used to the exercises. Calf muscle soreness and increased pain in the Achilles insertion may occur during the first 2 weeks of the programme.
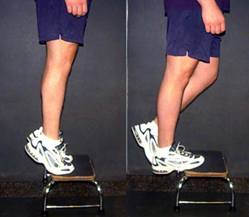
The Achilles Tendon Eccentric Stretch
- Stand on a step with both feet, with the balls of your toes on the step and with your heels off the step
- Keep your knees straight. Hold something if needed for balance
- Stand just on the painful leg
- Lower your painful heel down over the step, over a 2 second period. Hold the stretch for 5 seconds
- Now stand on the other leg, taking your weight off the painful side and push up, straightening your knee
- Bring the painful leg back onto the step, returning to the position in 1.
- This is 1 repetition (knee straight)
- Repeat 5 times in total
- Repeat the stretch again but with the knee slightly bent (20⁰)
- This is 1 repetition (knee bent)
- Repeat 5 times in total
- You have now completed a ‘set’ (10 repetitions done consecutively, 5 x knee straight, 5 x knee bent)
Week 1
Day 1-2 – 1 set of 10 repetitions (5 x knee straight + 5 x knee bent)
Day 3-4 – 2 set of 10 repetitions. 1 minute rest between sets
Day 5-6 – 3 set of 10 repetitions. 1 minute rest between sets
Day 7 – 3 set of 16 repetitions. 1 minute rest between sets
Week 2
3 set of 16 repetitions (8 x knee straight + 8 x knee bent). 1 minute rest between sets. Twice a day
Once 3 set of 16 repetitions can be completed with no pain or discomfort:
3 set of 16 repetitions wearing a ruck sac with 5 kg of books. 1 minute rest between sets. Twice a day
Continue to add weight in multiples of 5 kg if you do not experience pain in the Achilles tendon by the end of the third set.
Aim – to complete 3 sets of 16 repetitions with 1 minute of rest between sets, twice a day, 7 days per week, for 12 weeks.
The Achilles Tendon Eccentric Stretch
Extracorporeal Shock Wave Therapy (ESWT)
This is a non-invasive (does not breach the skin) treatment in which a device is used to pass inaudible, high-energy sound waves (shockwaves) through the skin, to the Achilles tendon. The exact way ESWT works is not fully understood, but the shockwaves may produce minor tissue damage. The body then produces a healing response and it is this that may lead to resolution of pain. ESWT is safe, although some minor side effects occasionally can be experienced, such as skin reddening, bruising or soreness. There is evidence that ESWT works and in combination with an Eccentric Stretching Protocol, it is better than eccentric stretches alone. Three separate treatments spaced approximately a week apart are normally required, each lasting about 5-10 minutes. Significant resolution of pain takes up to 2 months after completing treatment. Mr Gordon uses the Swiss DolorClast machine (by EMS), a state of the art device. ESWT is not normally available on the NHS. For private medical insurance purposes the treatment (CCSD) code is 3 sessions of T7250.
Surgical treatment
As a last resort, when the above treatments have not worked, certain surgical procedures can be performed on the Achilles tendon.
References
1. Alfredson H, Pietila T, Jonsson P, Lorentzon R Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26:360-6.
2. Kingma JJ, de KR, Wittink HM, Takken T Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. Br J Sports Med 2007;41:e3.
3. Rompe JD, Furia J, Maffulli N Eccentric loading versus eccentric loading plus shock-wave treatment for midportion achilles tendinopathy: a randomized controlled trial. Am J Sports Med 2009;37:463-70.
4. van Sterkenburg MN, van Dijk CN Mid-portion Achilles tendinopathy: why painful? An evidence-based philosophy. Knee Surg Sports Traumatol Arthrosc 2011;19:1367-75